OB/GYN Medical Billing Denial Management: How to Stop Losing Revenue to Claim Denials
If you run an OB/GYN practice, you already know that OB/GYN medical billing denial management is one of the most complex — and most costly — challenges you face. Denied claims don’t just create administrative headaches. They directly reduce your collections, strain your staff, and slow down cash flow at exactly the wrong moments.
I’m Jyoti, founder of RevantaRCM and a Certified Medical Billing and Coding Specialist (CMBS) with over 10 years working exclusively in medical billing. I’ve spent a significant portion of my career helping OB/GYN practices in Georgia, Florida, and Texas recover revenue they didn’t even know they were leaving on the table.
In this post, I’ll walk you through why OB/GYN practices get denied more than almost any other specialty, what the most common denial triggers are, and exactly what you can do to fix them.
Why OB/GYN Billing Has a Higher Denial Rate Than Most Specialties
OB/GYN practices deal with a unique combination of billing complexity that most other specialties don’t face. You’re managing global maternity packages, split care arrangements between providers, high-cost procedures that require prior authorization, and a constantly shifting payer landscape — all at the same time.
According to the Centers for Medicare & Medicaid Services (CMS), improper payments in fee-for-service billing remain a multi-billion dollar problem — and a large share of that stems from preventable coding and documentation errors.
In OB/GYN specifically, denials cluster around a few predictable areas. Once you know where they come from, you can stop them before they happen.
Global Maternity Package Confusion
Global OB packages (CPT 59400, 59510, 59610, 59618) are a major source of confusion and denials. When a patient switches providers mid-pregnancy, when a provider only delivers without providing antepartum care, or when services outside the global period are bundled incorrectly, payers push back immediately.
The fix requires meticulous tracking of antepartum visit counts, proper use of modifier -52 or -54 when splitting care, and clear documentation of delivery-only or postpartum-only scenarios. Many practices either skip this entirely or do it inconsistently — and payers know it.
Prior Authorization Failures
Many high-dollar OB/GYN procedures — including laparoscopies, hysteroscopies, and certain diagnostic imaging — require prior authorization. When your team submits a claim for a procedure that wasn’t authorized, or when the authorization on file doesn’t match the exact procedure code billed, you’re looking at an automatic denial.
I’ve seen practices lose tens of thousands of dollars annually just from authorization mismatches. The payer isn’t going to flag it for you — they’ll just deny it.
Diagnosis Code Specificity
ICD-10 requires a level of specificity that catches a lot of OB/GYN practices off guard. A vague or non-specific diagnosis code for a gynecological procedure — or using a code that doesn’t support medical necessity for the billed service — will result in a denial every time.
This is especially common with pelvic pain diagnoses, endometriosis management, and abnormal uterine bleeding. The clinical documentation has to back up the code, and the code has to align perfectly with the procedure.
The Most Common OB/GYN Denial Reasons (And How to Address Each One)
After years of working denial queues for OB/GYN practices, I’ve identified the denial categories that show up again and again. Here’s a practical breakdown.
1. Eligibility and Coverage Denials
This one is almost entirely preventable. When a patient’s insurance is verified at the time of scheduling but not re-verified on the date of service, you risk billing a payer that no longer covers that patient. Pregnancy is a life event that often triggers insurance changes — Medicaid enrollments, plan switches, new employer coverage.
What to do: Verify eligibility on every visit, not just at intake. Use your clearinghouse’s real-time eligibility tools and build it into your front desk workflow as a non-negotiable step.
2. Missing or Insufficient Documentation
Payers increasingly require clinical notes to support the medical necessity of certain procedures. If your documentation doesn’t clearly establish why a procedure was performed — or if the notes don’t match the billed codes — the claim gets denied or downcoded.
What to do: Train your providers to document the indication for every procedure, not just the procedure itself. If a hysteroscopy was performed because of abnormal bleeding that failed conservative management, that needs to be in the note — not just in the provider’s head.
3. Timely Filing Denials
Most commercial payers have a 90-day to 12-month timely filing window. Medicaid windows can be shorter. If your billing team is sitting on claims because of incomplete information, disputes, or staffing gaps, you may lose the right to bill entirely.
What to do: Implement a hard internal deadline of 30 days from date of service for all clean claims. Any claim held beyond 30 days should require a supervisor review with a documented reason.
4. Duplicate Claim Denials
These happen when the same claim is resubmitted without proper correction, or when an original claim and a corrected claim are both processing simultaneously. Payers flag these as duplicates and deny the second submission.
What to do: Always use the appropriate claim frequency code (bill type modifier) when resubmitting corrected claims. Track every claim by its original submission date and payer claim number.
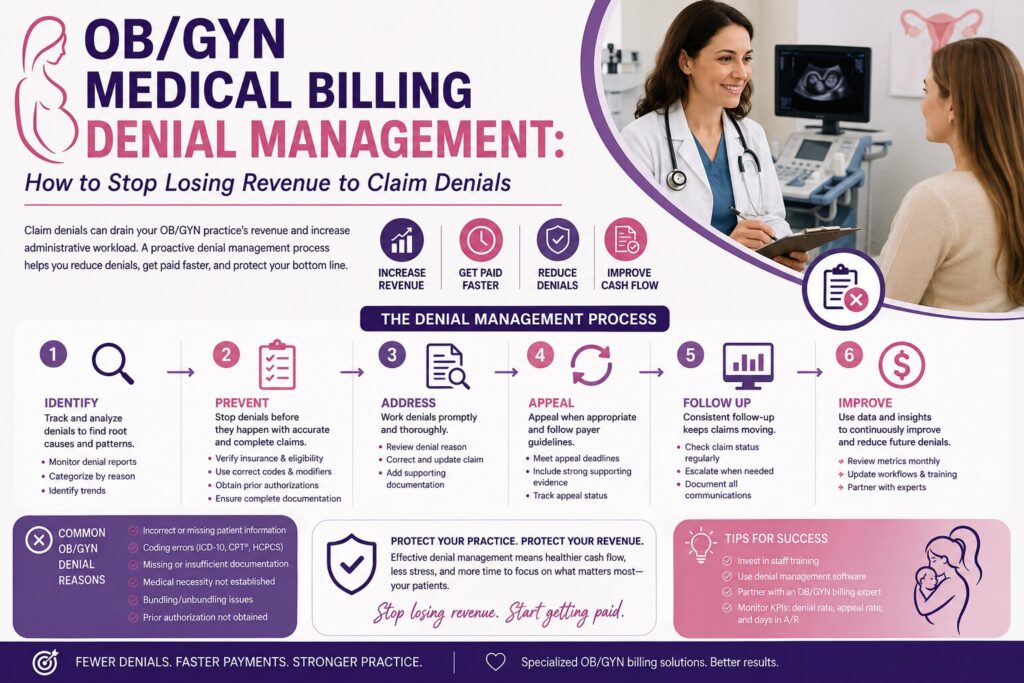
Building a Denial Management Workflow That Actually Works
Denial management isn’t a one-time fix — it’s a system. Here’s the framework I recommend for OB/GYN practices that want to get ahead of denials rather than constantly chasing them.
Step 1: Categorize Every Denial by Root Cause
Don’t just work denials individually. Every denial that comes in should be tagged by category: eligibility, authorization, coding, documentation, timely filing, or coordination of benefits. When you look at your denial data by category, you’ll quickly see where the patterns are.
Most practices are surprised to find that 60–70% of their denials trace back to the same 2–3 root causes. That’s where your process improvement energy should go.
Step 2: Set Denial Rate Benchmarks
The American College of Obstetricians and Gynecologists (ACOG) and industry groups generally consider a clean claim rate of 95% or higher a strong benchmark. If your first-pass acceptance rate is below 90%, you have a systemic problem — not just a staffing one.
Track your denial rate by payer. Some insurers deny at much higher rates than others, and knowing that helps you prioritize where to push back hardest.
Step 3: Appeal Every Appealable Denial
Many practices write off denials as uncollectible when they’re actually fully recoverable. If a claim was denied for incorrect documentation, and you can supply the correct documentation, appeal it. If a claim was denied for a coding issue that you can justify, appeal it with a letter of medical necessity.
The appeals process has timelines — usually 60 to 180 days depending on the payer and whether it’s a commercial plan or Medicaid. Don’t let those deadlines slip. A missed appeal deadline is permanent lost revenue.
Step 4: Close the Loop with Front-End Process Changes
The best denial management is denial prevention. Every time you successfully resolve a denial, ask: what process change would have prevented this claim from being denied in the first place? That question, asked consistently, is how practices reduce their denial rates over time.
See our full medical billing services to understand how we approach denial prevention from the first patient touchpoint through final payment.
What OB/GYN Practices in Georgia, Florida, and Texas Need to Know
State-specific Medicaid programs add another layer of complexity to OB/GYN billing. Georgia Medicaid (DCH), Florida Medicaid, and Texas Medicaid each have their own fee schedules, prior authorization requirements, and timely filing rules.
In Georgia, for example, the Department of Community Health administers Medicaid through managed care organizations with their own individual policies that layer on top of the base Medicaid rules. A denial that’s recoverable with one MCO may be non-recoverable with another for the exact same service.
If your practice operates across state lines or sees patients with out-of-state coverage, make sure your billing team is tracking payer-specific rules — not just applying a one-size-fits-all approach.
Frequently Asked Questions: OB/GYN Medical Billing Denial Management
What is the most common reason OB/GYN claims get denied?
The most common reason is eligibility and coverage issues — billing a payer that no longer covers the patient on the date of service. The second most common is prior authorization failures, particularly for surgical procedures. Both are largely preventable with front-end workflow improvements.
How long do I have to appeal a denied OB/GYN claim?
Appeal deadlines vary by payer. Most commercial insurers allow 60 to 180 days from the denial date. Medicaid plans often have stricter deadlines — sometimes as short as 30 to 60 days. Always check the Explanation of Benefits (EOB) for the specific payer’s appeal instructions and deadline.
Can I bill separately for services included in the global OB package?
Generally, no — unless those services fall outside the global period or are clearly outside the scope of the global package. Examples include significant, separately identifiable E/M visits (billed with modifier -25), complications management that requires additional resources, or services clearly unrelated to the pregnancy. Always document the medical necessity and use the appropriate modifiers.
What denial rate should my OB/GYN practice be aiming for?
Aim for a first-pass clean claim acceptance rate of 95% or higher. A denial rate consistently above 5–8% suggests systemic issues in your coding, eligibility verification, or authorization workflow that need to be addressed at the root cause level.
Is it worth outsourcing OB/GYN denial management?
For most practices, yes — especially if your in-house team is spending more time working denials than preventing them. A specialized billing partner who understands OB/GYN coding nuances can often recover significantly more revenue than internal teams while simultaneously reducing future denial rates.
Ready to Stop Losing Revenue to Denials?
Denial management isn’t something you have to figure out alone. At RevantaRCM, we specialize in OB/GYN billing and we know exactly where the revenue leaks are — because we’ve fixed them for practices just like yours in Georgia, Florida, and Texas.
Whether you need a full denial audit, an appeals workflow overhaul, or end-to-end billing support, we can help. Contact us today for a no-obligation consultation. Let’s find out exactly how much your practice could be recovering.